
Redetermination/Reopening Form Tutorial - JE Part A
Redetermination/Reopening Form Tutorial
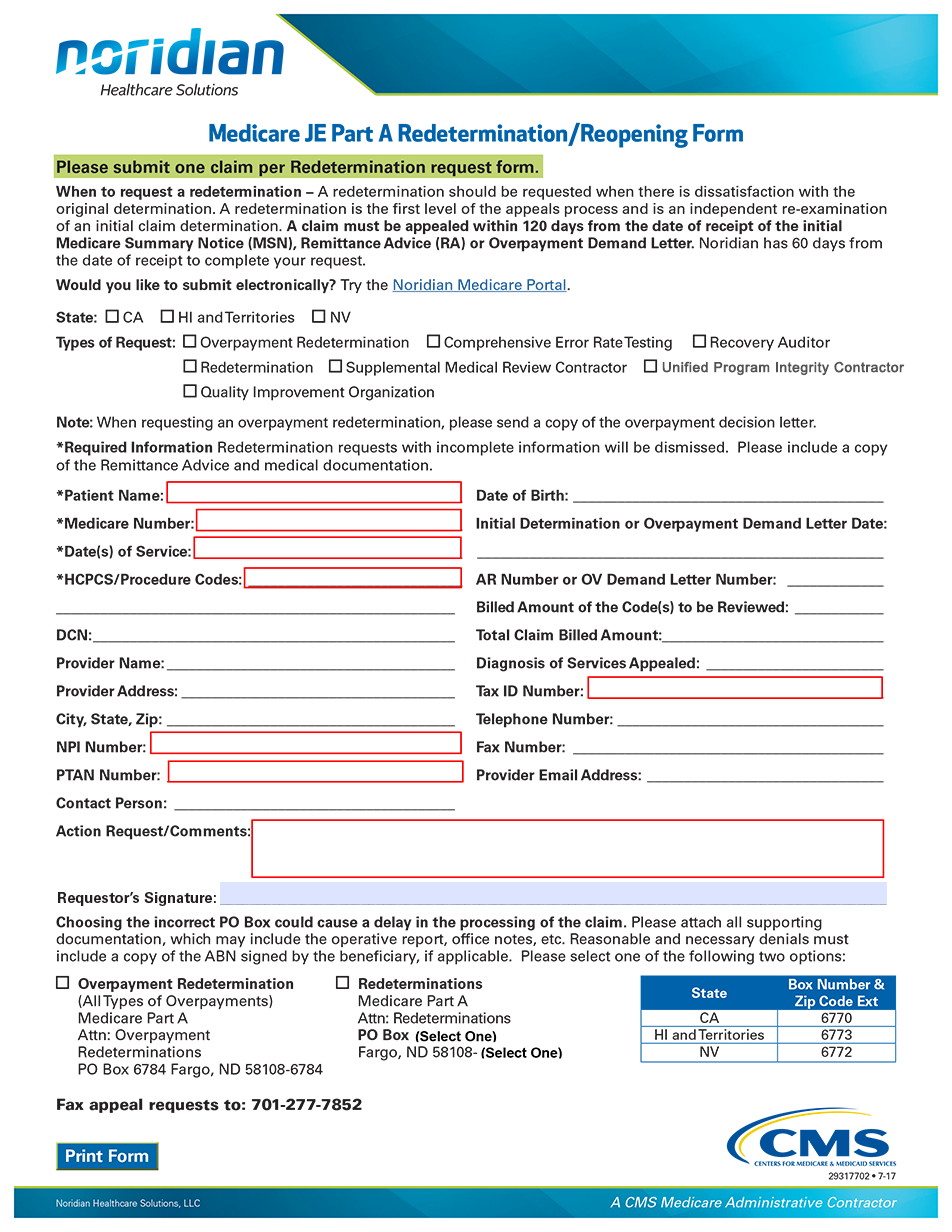
Move your cursor over any field in the interactive form below; you'll see instructions on how to complete the field. You may also click in any field for more detailed instructions.
Last Updated Mar 28 , 2022
